
Procedure: Chemical Peel and Lower Face Liposuction
Cosmetic Concern:
68-year-old woman who is unhappy with her saggy lower eyelid bags and aging face.
Diagnosis:
1. Malar festoons (bags)
2. Aging face
3. Jowling
Treatment:
1. Full-face chemical peel
2. Lower face and neck liposuction
Discussion:
Note the dramatic improvement in the quality of her skin and the contour of her lower face. She had 8 days of down time with her procedures. A lower face lift would have made a bigger difference, but this patient did not want the down time or the need for a general anesthesia. Her procedure was accomplished in the office procedure suite under local anesthesia! Learn if this treatment would be right for you by calling to schedule your personal consultation with Dr. Steinsapir.

Procedure: Full Face Chemical Peel
Cosmetic Concern:
52-year-old woman unhappy with the fine wrinkles around the mouth and lower eyelids. She also is bothered by the sun freckles and a general yellowing of her complexion. She had several girl friends that had CO2 laser resurfacing. She felt that their results were unnatural and she was interested in alternatives to laser resurfacing.
Diagnosis:
1. Lower eyelid wrinkles and herniated orbital fat
2. Upper lip wrinkles (smoker’s lines)
3. Generalized sun damage
Treatment:
1. Full-face chemical peel
Discussion:
Her chemical peel was individualized and tailored to her needs. The lower eyelid and perioral area were peeled more deeply than the surrounding facial areas. The chemical peel of the lower eyelids has the capacity to stimulate enough new collagen formation to help flatten the under eye circle as well as smoothing the lower eyelid wrinkles. The after picture was taken 4 years after her chemical peel. Dr. Steinsapir is a master chemical peeler. Thanks to his innovative approach, this peel can be comfortably performed under local anesthesia in the office procedure suite. Her skin was intact and ready for make up in 8 days.
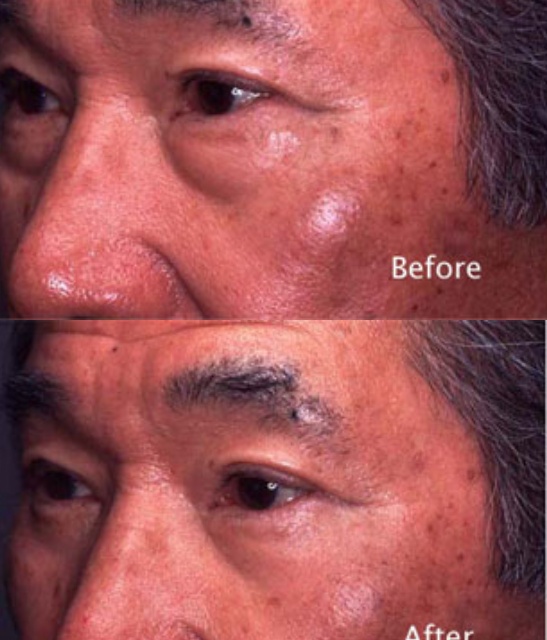
Procedure: image
Lower Eyelid Chemical Peel and Lower Eyelid Surgery
Cosmetic Concern:
59-year-old man bothered by the fullness in the lower eyelids.
Diagnosis:
1. Herniated lower eyelid fat
2. Lower eyelid wrinkles
3. Sun damaged skin
Treatment:
1. Transconjunctival lower eyelid surgery
2. Lower eyelid chemical peel
Discussion:
Lower eyelid surgery reduced the fullness of the lower eyelid by removing eyelid fat. This tends to deflate the lower eyelid and slightly increase the lower eyelid wrinkles. The chemical peel performed at the time of the lower eyelid surgery, helps to firm the lower eyelid skin and reduces this tendency and avoids the need for surgery to remove any excess lower eyelid skin.

Procedure: Full Face Chemical Peel
Cosmetic Concern:
This 75-year-old woman had a long-standing history of sun damage to her face. She was looking for a treatment that would make a significant difference without requiring her to undergo general anesthesia.
Diagnosis:
1. Severe sun damaged skin
2. Marked facial wrinkles
3. Aging face
Treatment:
Individualized full-face chemical peel under local anesthesia in the office. By individualizing a chemical peel to meet her needs, she had the maximum benefit and was able to wear make up just eight days after her chemical peel. Dr. Steinsapir has developed a unique peeling method that comfortably permits a major chemical peel with minimal anesthesia in the office procedure suite. Call now to learn if this treatment is right for you.

Procedure: Upper Face Lift & Chemical Peel
Cosmetic Concern:
51-year-old woman who is interested in a more youthful appearance.
Diagnosis:
1. Bilateral eyebrow ptosis
2. Lower eyelid wrinkles
3. Herniated orbital fat
Treatment:
1. Endoscopic forehead lift
2. Lower eyelid chemical peel
Discussion:
The endoscopic forehead lift needs to be tailored to the desires of the individual patient. She did not want the “deer in the head light” look that can result if the eyebrow is overly elevated. She also wanted to have something done for the lower eyelid but budget was a major consideration. A chemical peel of the lower eyelid complex was the logical choice for treating the lower eyelid. Even though no surgery was performed on the lower eyelids, the chemical peel firms the lower eyelid septum smoothing the area. This is often a great option as an alternative to lower eyelid surgery or arcus marginalis release. Call now for your personal consultation to learn if these procedures are right for you.

Procedure: Full Face Chemical Peel
Cosmetic Concern:
55-year-old woman with fine wrinkles around the mouth. She is also bothered by the sun freckles, a general yellowing of her complexion, and the way her lipstick runs in the lines around the mouth. This is called lipstick bleed.
Diagnosis:
1. Lower eyelid wrinkles
2. Upper lip wrinkles
3. Generalized sun damage
Treatment:
1. Full-face chemical peel
Discussion:
Her chemical peel was individualized and tailored to her needs. The lower eyelid and perioral area were peeled more deeply than the surrounding facial areas. The after picture was taken 7 years after her chemical peel. Dr. Steinsapir is a master chemical peeler. Thanks to his innovative approach, this peel can be comfortably performed under local anesthesia in the office procedure suite. Her skin was intact and ready for makeup 10 days after her chemical peel.