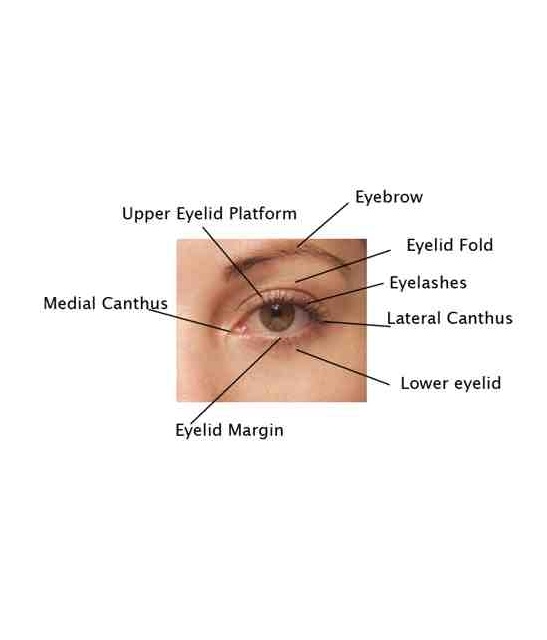
Eyelid
Upper Eyelid Platform
Eyebrow
Eyelashes
Lateral Canthus
Lower Eyelid
Eyelid Margin
Medial Canthus
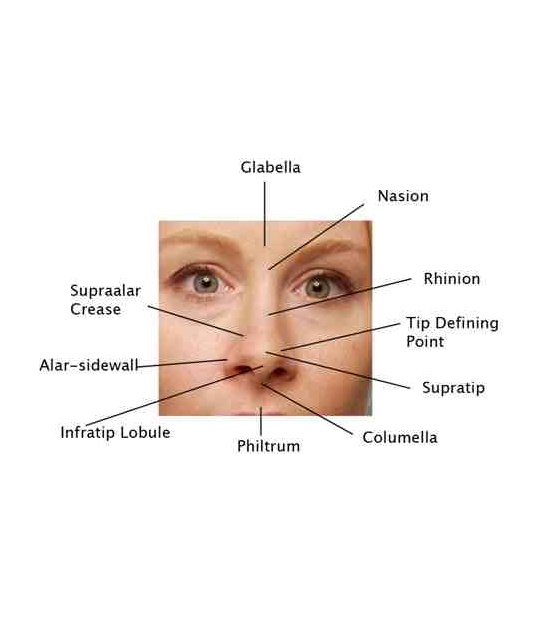
Front of Face
Glabella
Nasion
Rhinion
Tip Defining Point
Supratip
Columella
Philtrum
Infratip Lobule
Alar-Sidewall
Supraalar Crease
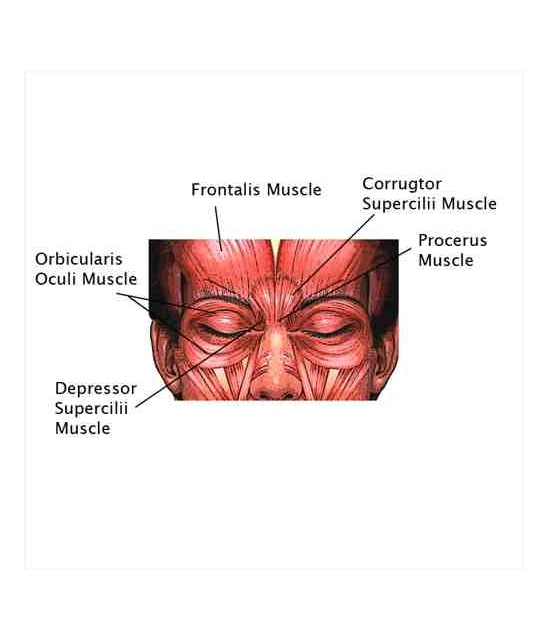
Facial Muscles
Frontalis Muscle
Corrugtor Supercilii Muscle
Procerus Muscle
Depressor Supercilii Muscle
Orbicularis Oculi Muscle
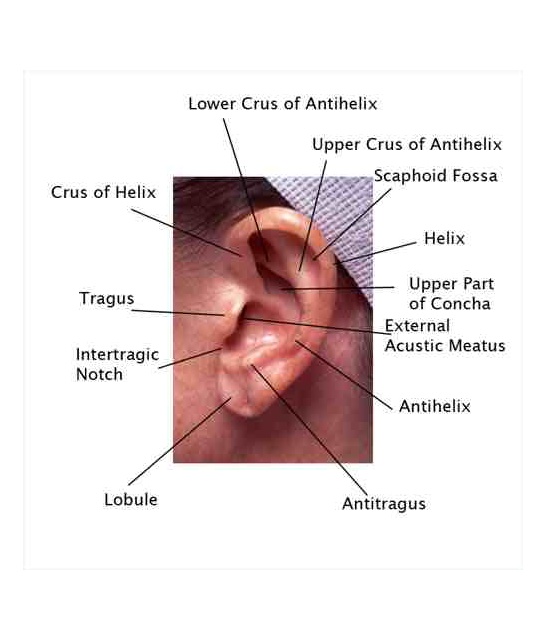
Ear
Lower Crus of Antihelix
Upper Crus of Antihelix
Scaphoid Fossa
Helix
Upper Part of Concha
External Acustic Meatus
Antihelix
Antitrugus
Lobule
Intertragic Notch
Tragus
Crus of Helix